This is really part 2 of a “catch-up” series on what I’ve been researching and thinking about recently that started with yesterday’s, “What Do I Know Now That I Didn’t Know Then?“.
For anyone trying to manage their pre- or full- diabetes through diet and exercise, there are two points I want to make. BTW, by manage I mean keeping your blood sugar below the level at which irreversible retinopathy, neuropathy and all the other opathy’s occur as well as avoiding an early demise. So the points are:
- Low carb vs low fat is a false dichotomy. The diet answer lies elsewhere and has been known for years and might just be an “inconvenient truth” that the food industry does not want you to know.
- The order in which you eat the food items on your plate could just make the difference between winning and losing the battle against the opathy’s.
Here’s how I came to these conclusions …
Pubmed
Having good reason to believe that I wasn’t insulin resistant, but was still unable to handle glucose, I started searching pubmed to see what I could find. Almost immediately, I discovered a new (to me) diabetic category: Latent Autoimmune Diabetes in Adults (LADA), which accounts for about 5% – 10% of diabetics. LADA is like T1 diabetes, but it develops later in life, without necessarily developing obesity and insulin resistance first. This was a really interesting discovery, since I could never understand how I could be diabetic and not have any of the lifestyle risk factors.
But although it was interesting, it wasn’t what I needed to know, ie, what’s the best diet for people with insufficient insulin production? I recalled that Plant Positive (PP) had some videos that might apply, and I knew that I could count on him to make the strongest possible case for veganism and probably for high carb. Two points stood out from the last of a number of his videos that I watched.
A Plant Positive Video
First, diabetes cannot be blamed on too many carbs or obesity. The experiment that proves it? Two lean men ate nothing but meat for a year. At the end of the year, one of the men had sugar in his urine, and so, would be diagnosed as diabetic. So, he certainly didn’t overdo the carbs and although the journal article doesn’t say whether or not he became obese, it seems doubtful that a) he would become obese on a meat only diet and b) he would do so and it wouldn’t be reported. And the clincher was, after he returned to his normal diet, his glucose metabolism also returned to normal.
Here’s a screen shot from the journal article showing the 2 glucose tolerance tests (OGTT), one (upper, solid line) at the end of the year-long meat-fest and the other after he adjusted back to a more normal diet:

The disturbing part for me in seeing this was how similar that solid upper line is to my OGTTs (see part 1). The magnitude of the numbers is the same as mine. Does this means I probably have sugar in my urine too? But the good news is, maybe mine is just as reversible as the study subject’s was. The baffling part for me in this was I wasn’t eating an all meat diet; I was trying to increase the carb content of my diet from about 30% to 50%. It makes no sense.
The second point that grabbed me was that PP was in agreement with Evelyn aka CarbSane that free fatty acids (FFA) might contribute or even be responsible for insulin resistance. From PP’s video:
Back in 1963, low-carb diets were investigated for their effects on free fatty acids and blood glucose. These researchers studied normal people as well as diabetics.
In the normal people, insulin, free fatty acids, and glucose all soared after carbohydrate restriction. These researchers saw a parallel between carbohydrate restriction and diabetes.
…
Insulin and blood glucose returned to normal after their diets added back carbs.
So, the good news is that, at least in this 5-day instance, low-carb diet induced glucose metabolism dysfunction was reversible, as was the case for the year long meat diet. The bad news is the problem with a low carb diet is even worse than PP reported, at least in my eyes. I went to the original journal article and found that the researchers reported that after 5 days on a 50g / day low-carb diet, gluco-normal men’s fasting FFAs had more than doubled, so as to be well into the range of diabetic fasting FFA. With a good possibility that these elevated FFAs are indeed toxic to beta-cells, I’m really glad I never went for the very low version of low-carb.
A Portugeuse LADA Study
OK, so I get from this that for gluco-normal people and people with insulin resistance, carb restriction might be a really bad idea. But what about people who aren’t normal or insulin resistant, ie type I or type 1.5 diabetics (as LADA is sometimes called)? Is carbohydrate restriction beneficial or detrimental? According to this, using insulin to reduce demand on beta cell function has a preservative effect on the beta cells:
The use of insulin reduces the activity of beta-cells, antigen expression and decreases the autoimmune process, with consequent reduction of cell destruction
…
By early insulinization of diabetic patients over 35 years and GADA> 20 U / ml, we observed that there was, during the follow-up of 48 months, significant changes in C-peptide levels, indicating preservation of beta-cell function
So why wouldn’t the reduced demand on beta cell function achieved by a lower carb diet work equally well?
Well, one answer might be that the carb calories have to be replaced with something. If they are replaced in part by protein, per gram, protein evokes an even greater insulin response from the beta cell than do carbs. So it is clear that if any benefit is to be realized, fat, not protein must be substituted for the fewer carb calories. But, we’ve learned that the fatty meal is going to elevate free fatty acids levels which will lead to beta cell loss just as much as elevated serum glucose will. It’s looking like that rock and hard place all over again.
Beans, beans, the magical fruit!
I was feeling very discouraged until I found this. It’s a podcast presentation from the 2013 EASD Annual Meeting in Barcelona. The EASD is the European Association for the Study of Diabetes. The talk, delivered by Prof. Jim I Mann who, BTW, actually did some of the landmark studies he discusses, totally clears up certain dietary confusions — confusions which may have been intentionally created by the food industry. Back in the day, the question for diabetes, it seems, was never about low carb vs high carb; it was about low carb vs high soluble fiber. That question was totally answered back in 1981 with a study by Simpson et al published in the Lancet. The results speak for themselves:

HL = high leguminous fiber diet, LC = low carb

Low carb (solid line above) vs high legume, 24 hour BG
But, if numbers and charts make your head spin, I will explain. The top slide shows the bean diet (HL) reducing bad cholesterol (LDL) by about 20% down to just about 100 mg/DL (in US numbers). The slide on the bottom shows the utter superiority of the bean diet for 24-hour glucose control.
These results have been replicated time and again, in studies all over the world, in all kinds of permutations and combinations, and with type I, type II, pre, whatever diabetics. The high soluble fiber diet wins hands down in every measure of diabetic and serum lipid control, as well as achieving a 44% reduction in CHD and overall mortality for type I diabetics in this 2012 study (see “Tertiles of Sol fibre” on the right):

“Whole Food” concept re-examined
The rest of the podcast presentation clears up a confusion regarding the fact that all high carb diets are not created equal when it comes to BG control. The imperative regarding carbs in your diet is that not only must they be high in soluble fiber, but also, whatever processing was done to the food, the cellular structure must not have been disrupted. So for instance, even if your bread claims to be organic, non-GMO, whole grain and stone ground, if it’s not hard and dense enough to serve as a ship’s anchor, you shouldn’t be eating it.
Here’s the study that he described as being the most important of all, comparing the effect on BG throughout the day of 2 diets with the same amounts of carb and fiber. The difference was the cellular structure of carbs in the diet corresponding to the triangles (lower line) had been left intact, whereas for that of the other diet – because the beans, whole grains, etc, had been ground up – it was destroyed.
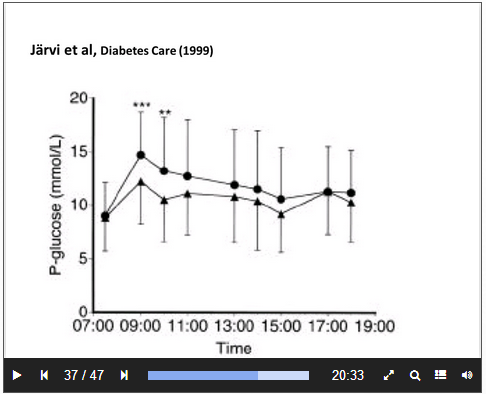
Triangles (lower) = minimally processed carbs
Lipid levels were similarly improved, although I haven’t reproduced the slide here.
As an aside from the EASD podcast, here is a widely cited 2012 paper that I had read quite a while ago that supports this concept of “whole foods”. But it is whole foods not in the sense that nothing has been removed, but that the food has been left whole, ie, intact. The paper examines the effect of eating foods whose cellular structure is no longer intact: Comparison with ancestral diets suggests dense acellular carbohydrates promote an inflammatory microbiota, and may be the primary dietary cause of leptin resistance and obesity and a very interesting chart from that paper. Even if you don’t want to read the whole paper, the chart will definitely give you something to think about.
Dietary Recommendation Summary
The concluding dietary recommendations for diabetics from the podcast is that we aim for low GI, but that this leaves too much wiggle room for people to, perhaps willfully, misinterpret. How is a net low GI meal achieved? To be more specific:
- Carb intake can be 40% – 60% of calories, as tolerated by your glucose metabolism.
- Simple sugars can be up to 50 grams/day as tolerated by your glucose metabolism.
- Fiber intake should be at least 40 grams/day, aiming for mostly soluble fiber.
- Fiber must not be ground up, extracted or synthesized in the lab.
- Fiber should not be listed as an ingredient.
- Cellular structure must remain intact, thus eliminating most whole grain breads and cereals.
- Carbs from legumes, pulses and “genuine” whole grains are best.
- Avoid starchy vegetables, cereals and grains, such as rice, potatoes, most breads.
Meal item order makes a huge difference – original research
I was very excited by all this information. I had done my diet experiment all wrong. I thought the higher carb part gave me license to eat all the stuff I had been avoiding while I was eating low carb, as long as I didn’t put in any added sugar. I wanted to give it another try, this time building around beans, raising my carb intake very gradually and as a final twist, I came up with the idea that, wherever possible, I would try eating my beans (or other carbs) after I ate the protein and fat portion of the meal.
It had taken me 11 days to find that podcast. The morning of April 12, for breakfast (breakfast is always the most problematic meal) I replaced my (fluffy) 100% organic sprouted whole grain bread with beans that were eaten last . The result? I was absolutely blown away by how low my 50 min BG was (114)! I didn’t really trust it, so I repeated the exact same meal for the next 3 days with BGs of 102, 104, 103.
Long story short, it finally occurred to me that the order in which I ate the food items in the meal might actually making the biggest contribution to those low numbers. I started switching the order every other day on the same breakfast. The meal is about 31-17-21 (%P – %F – %C). Here’s my result for a month:
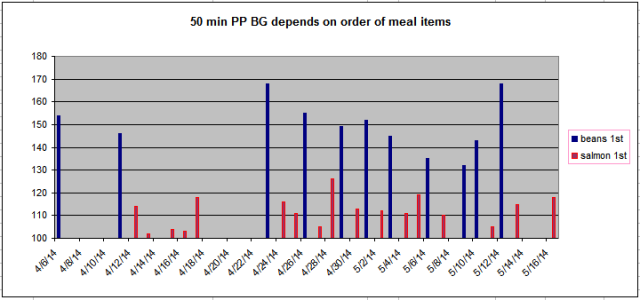
So, again, if charts make your eyes lose focus and glaze over, I will explain. All those bars represent days for which I had the (almost) exact same breakfast and got a valid glucometer reading within a few minutes of 50 from the start of my breakfast. The blue bars represent my readings on the days that I ate my beans first and then followed them with a salmon patty and avocado. The average BG reading for the blue days is 147. On the red bar days, I ate my salmon and avocado first. The average for those days is 112.
Why is this significant? Because right around 140-150 mg/dl is where irreversible opathy damage starts to occur. Yes, I know that Evelyn (aka CarbSane) thinks Jenny (Blood Sugar 101) pulled this number out of her you-know-where, but surely some of the many studies mentioned here have merit. And right around 110? That’s where a gluco-normal person’s blood sugar would be.
BTW, I haven’t seen this result mentioned anywhere and was wondering if it could be replicated. I was sorta hoping I could get one of my diabetic or pre-diabetic readers to try a similar experiment with meal item order and report back.
Meanwhile, next in this series, I’ll be sharing some very interesting journal article finds.






 I find it flabbergasting that people can be convinced that all those extra pounds are benign, much less healthy, so I decided to look into it to see if maybe I was wrong and they were right. Here’s just the tip of the iceberg of what I found. (Spoiler: it doesn’t support the obesity deniers.)
I find it flabbergasting that people can be convinced that all those extra pounds are benign, much less healthy, so I decided to look into it to see if maybe I was wrong and they were right. Here’s just the tip of the iceberg of what I found. (Spoiler: it doesn’t support the obesity deniers.)











